Environmental Cadmium Exposure Induces Kidney Tubular And Glomerular Dysfunction in The Myanmar Adults
May 07, 2022
For more info. contact tina.xiang@wecistanche.com
ABSTRACT—Cadmium is an environmental toxic metal and its exposure has become a worldwide public health threat. We aimed to evaluate the exposure assessment of cadmium in people living in Ta Zin Yae Kyaw village of Nyaung Don Township in Ayeyarwady Division, Myanmar, and the adverse effects of cadmium on the kidneys. Subjects(18-40 years)residing in this village were selected as the exposed group (n=65)and those living in Kamayut Township in Yangon Division, Myanmar as the control group (n=65)Spot urine samples were taken to the determination of urinary cadmium concentration using graphite-furnace atomic absorption spectrometry(GFAAS)method and adjusted to the concentration of creatinine in urine. To assess the kidney function, urinary β,-microglobulin level was determined by ELISA, serum creatinine was measured by colorimetric Jaffe method, and estimated glomerular filtration rate(eGFR)was calculated by Chronic Kidney Disease Epidemiology Collaboration(CKD-EPI)equation. Urine cadmium concentrations were significantly higher in the exposed group (median (Interquartile range):0.96 (0.19-1.77)ug/g Creatinine)compared to the control (p =0.036).Urinary β,-microglobulin levels were significantly higher(p= 0.000)and eGFR was significantly lower in the exposed group (p= 0.013)compared to the control. In addition, urine cadmium levels showed a significant positive correlation with urinary β,-microglobulin in all study populations (p<0.01). The positive correlation becomes stronger(p<0.01)in the exposed group only. For eGFR, a significant negative correlation was found in all study populations (p<0.01)and the exposed groups (p<0.01). Our findings suggested that environmental cadmium exposure can induce renal dysfunction in both tubular and glomerular functions in apparently healthy human adults.
Keywords: Cadmium, Kidney tubular function, Kidney glomerular function, Adults, Human

Click to learn cistanche tubulosa adalah and cistanche for sale
INTRODUCTION
Cadmium, a toxic heavy metal, is mainly a by-product of zinc mining, smelting, and refining. Residues of coal combustion, mine tailing, urban refuse, smelter slag, and waste are deposited on lands through atmospheric emissions(Faroon et al,2012)and thus the appliance of cadmium-containing fertilizers and sewage sludge on farmland may cause the contamination of soils, and cadmium uptake is increased by crops and vegetables grown for human consumption(Jarup and Akesson,2009). Diet is the main source of environmental cadmium exposure in most parts of the world. Cadmium in drinking water contributes only to but a small percent of all cadmium intake (Olsson et al,2002). Tobacco smoking is another important source of cadmium exposure (McElroy et al,2007). Cadmium concentrations in ambient air are generally low. In areas with contaminated soils, house dust is potentially an important source of exposure to cadmium, even after the closure of the cadmium-emitting source(Hogervorst et al,2007).
Cadmium exposure is associated with nephrotoxic effects, particularly at a high exposure level (median urinary cadmium(UCD),13.5ug/g creatinine)(Jarup et al., 1993). However, some studies of cadmium expo-sure and its health impact on human populations reported that adverse effects may occur even at lower exposures (Jarup et al,1998; Menkeet al.,2009; Eom et al.2017). In addition, numerous studies have reported health effects of cadmium exposure in the general population, also in
the absence of specific industrial exposure (Jarup and Akesson,2009).
Although previous research has focused on the kid-ney (as cadmium is nephrotoxic) and bone(causing osteoporosis), a recent study has also reported cancer risk in lungs, kidney, and prostate at low-level environmental exposure(Jarup and Akesson,2009), cadmium-associated pulmonary diseases such as chronic obstructive pulmonary disease and emphysema(Lampe et al,2008), a cardiovascular disease especially for coronary heart disease (Tellez-Plaza et al, 2013), and acute central and peripheral neurotoxicity (Ismail et al,2015).
Kidneys are the main organ to be affected by cadmium in long-term exposure(Boonprasert et al,2011). Cadmium is well retained in the kidney(half-life: 10-30 years), and the urinary cadmium concentration is mainly influenced by the body's burden of cadmium. Thus, the amount of cadmium in the urine shows both recent and past exposure, whereas the amount of cadmium in the blood shows recent exposure to cadmium. Cadmium levels in hair or nails are not as useful as an indicator of when or how much cadmium may have been taken in, partly because cadmium from outside of the body may attach to the hair or nails(Agency for Toxic Substances and Disease Registry (ATSDR),2012).
Initially, exposure to cadmium causes kidney tubular damage. Elevations in the excretion of low molecular weight proteins, such as β,-microglobulin,α,-microglobulin, or retinol-binding protein, have been used as indicators of damage to the tubular protein absorption capability. After prolonged and /or high exposure, the tubular injury may progress to glomerular damage with decreased glomerular filtration rate(GFR), and eventually to renal failure (Jarup and Akesson,2009; Johriet al.,2010).In a previous in vivo study, low-dose cadmium exposure induced overproduction of the interstitial matrix component fibronectin and the expression of the myofibroblasts/EMT(epithelial-mesenchymal transition)marker α-SMA in kidneys of mice, which might lead ultimately to renal fibrosis (Thijssen et al,2007).
In Myanmar, environmental heavy metal exposure is an emerging public health issue. But there is limited evidence for public health data concerning the cadmium-contaminated areas. A previous study reported on the relationship between prenatal heavy metal exposure and adverse birth outcomes in pregnant mothers residing in Ayeyawady Division(Kyi-Mar-Wai et al.,2017). In that study, they identified that pregnant mothers were highly exposed to cadmium(the median value of adjust-ed urine cadmium level was 0.9μg/g of creatinine). Accordingly, a pilot study was done on apparently healthy male and female subjects living in Ta Zin Yae Kyaw village, Nyaung Don Township, Ayeyarwady Division to evaluate the exposure assessment of cadmium. It was found that there might have been low cadmium exposure, although the drinking water sample for the inhabitants has no cadmium contamination. Therefore, the study of the effects of cadmium should be done on these apparently healthy people. The present study aimed to evaluate the exposure assessment of cadmium in people living in those areas and the adverse effects of cadmium on the kidneys.

MATERIALS AND METHODS
Study area and subjects
This study was carried out from December 2018 to September 2019. In the present study, apparently healthy participants, aged 18-40 years, residing in the Ta Zin Yae Kyaw village of Nyaung Don Township in Ayeyarwady Division, Myanmar, were selected as the exposed group (n=65)(Fig. 1)and those residing in Kamayut Township in Yangon Division, Myanmar as the control group (n =65). Adult male and female subjects were selected from these areas. They were requested to come to the local authority offices and the detailed procedure, aim, and objectives of the study were explained. Then they were asked for their voluntary participation. Written informed consent was taken from the volunteers. Those with body mass index>25 kg/m2, known history of renal diseases or urological diseases, hypertension or diabetes, blood pressure≥140/90 mm Hg, random blood sugar≥180 mg/dL or 10 mmol/L, and female subjects with pregnancy were excluded. A total of 130 subjects participated in this study. Spot urine samples and blood samples were taken for biochemical analysis.

Collection of samples and biochemical analysis
Subjects were requested to collect a spot urine sample using a clean beaker provided. It was transferred to a 50 ml polyethylene bottle and two 5 mL urine tubes:50 mL bottle for analysis of urinary cadmium, one 5 mL tube for β-microglobulin within 7 days after collection, and the other 5 mL tube for measurement of creatinine level. Prior to storage, one drop of 0.5 N sodium hydroxide was added to this tube to adjust the urine pH to 6-8 to prevent further degradation of β-microglobulin in an acidic condition. The urine samples were transported in a cool box. The samples for detection of urinary cadmium levels were forwarded to the laboratory of the Occupational and Environmental Health Department within 24 hr of collection. The remaining two samples were stored at-20°C in the Postgraduate Research Laboratory, Physiology Department, University of Medicine 1, Yangon, for biochemical analysis.
Three mL of peripheral blood was taken from the ante-cubital vein under aseptic condition and it was collected in a test tube with no anticoagulant for determination of serum creatinine. The blood sample was also transported in a cool box. It was centrifuged at 2000 rpm for 10 min. The serum sample for creatinine was stored at-20°C.
The urinary cadmium was measured by the graphite furnace atomic absorption spectrometry(GFAAS)meth-od.β,-microglobulin in urine was measured by Enzyme-linked Immunosorbent Assay (ELISA)(EIA-1789. DRG International, Inc., Springfield, NJ, USA). The levels of creatinine in serum and urine were measured by the colorimetric Jaffe method using a commercial kit(auto-Creatinine liquid color, Wiesbaden, Germany). To adjust the spot urine samples for dilution, all urine parameters were adjusted to the concentration of urinary creatinine(UCR). Individual subject glomerular filtration rate (eGFR, in milliliters per minute per 1.73 m2)was estimated from their serum creatinine, age, and gender using the CKD Epidemiology Collaboration(CKD-EPI)formula: CKD-EPI GFR = 141 x min(Scr/k,1)x max (Scr/k,1)-1.20x0.993Agx 1.018 [if females x 1.159 [if African American], where Scr is serum creatinine(mg/dL), K is 0.7 for females and 0.9 for males,α is-0.329 for females and-0.411 for males, min indicates the minimum of Scr/k or 1, and max indicates the maximum of Scr/k or 1(Levey et al.,2009).
Statistical analysis
All calculations were performed using computer-based SPSS software version 22 and the master sheet then was counterchecked. Descriptive statistics of numerical variables with normal distribution were expressed as mean ± SD and those with skewed distribution as the median and interquartile range(IQR). Descriptive statistics of categorical variables were expressed as frequency and percentage. Z-test and Student's t-test were used to compare categorical and continuous data. The Chi-square test was used to compare categorical variables. The comparison of renal parameters between chronic cadmium-exposed and control groups was performed using the Mann-Whitney U test. Spearman's correlation coefficient (rho) was used to evaluate a correlation between urinary cadmium and renal parameters. Pvalue<0.05 was considered statistically significant.
Ethical consideration
This study was carried out according to the ethical guideline issued by the Research and Ethics Committee of University of Medicine 1, Yangon after getting permission from the local authority(073/UM1, REC.2018). The individual was invited for voluntary participation.

RESULTS AND DISCUSSION
The general characteristics of the 130 study subjects(65 in the exposed group and 65 in the control group)are presented in Table 1. The mean age was higher in the exposed group(29.86±6.46 years)than in the control group (21.7±5.20 years). The mean body mass index (BMI) was not different between the exposed group and the control group. The proportions of smokers and betel quid chewers were higher in the exposed group than in the control group. In the present study, the median urinary cadmium level of the subjects was significantly higher (p=0.036) in the exposed group(0.96ug/g Cr)than in the control group(0.41 μg/g Cr)(Table 2). It was found that urinary β-microglobulin level was significantly higher (p =0.000)in the exposed group compared to the control group, and eGFR was significantly lower in the exposed group (p=0.013)compared to the control group(Table 2).

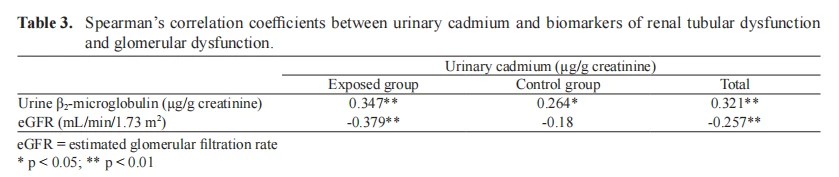
In addition, the correlations between urinary cadmium and biomarkers of renal tubular and glomerular function in all study populations, the exposed group, and the control group, are shown in Table 3. There was a significant positive correlation between urinary cadmium lev-el and urinary β,-microglobulin in the study population (Spearman's rho= 0.321, n= 130,p<0.01)(Fig.2). When it was studied in the exposed group only, the correlation becomes stronger(Spearman's rho =0.347,n=65, p<0.01), although a significant positive correlation was also found in the control group(Spearman's rho=0.264, n=65,p<0.05)(Fig.3).Likewise,there was also a significant negative correlation between urinary cadmium level and eGFR (Spearman's rho =-0.257,n= 130,p<0.01)(Fig. 4). A similar pattern but a stronger negative correlation was found in the exposed group only (Spearman's rho=-0.379,n=65,p<0.01)(Fig.5).




Although most of the previous Myanmar studies concerning the health effects of heavy metal exposure were focused on lead, arsenic, and mercury, studies on cadmium-related health effects are still limited in this country. In Ayeyarwady Division, the southern region of Myanmar, the groundwater is confirmed to be highly contaminated with arsenic(Tun,2003), but data for cadmium was not known. This region plays a central role in the cultivation of rice in rich alluvial soil. Rice has been identified as one of the major sources of cadmium and leads intake in humans, especially in Asia. Up to 50% of the ingested cadmium was from rice and its products in Asian countries (Tsukahara et al,2003). It was found that cadmium is present in brown rice and white rice produced from the Ayeyarwady region (Phyo-Wai-Zin et al.,2018).
In the present study, urine cadmium concentrations of 130 subjects were measured and it was found that the median value of urinary cadmium in the exposed subjects was 0.96 μg/g of creatinine. It was consistent with a previous study (the median value of adjusted urine cadmium lev-el was 0.9 μg/g creatinine) done in the Ayeyawady region, Myanmar(Kyi-Mar-Wai et al.,2017). However, it was higher than those reported for an Asian population (median,0.59 μg/g creatinine)(Kippler et al.,2007). The cadmium concentration of the exposed subjects in the present study(median, 0.96 μg/g creatinine) was comparatively higher than the normally acceptable level in human subjects(0.19 ug/g creatinine)(ATSDR.2008). According to ATSDR(2012), a urinary cadmium concentration of more than 5ug/g of creatinine is regarded as high exposure. Thus, it could be assumed that the populations in the present study were exposed to low doses of cadmium(ATS-DR, 2012).
The general characteristics of the subjects in the exposed group were more or less similar to those in the control group in all aspects. Moreover, the subjects in both groups were predominantly young, non-obese, and apparently healthy, so they had a low risk of renal diseases. However, the mean age of subjects in the exposed group was higher than the control group. Only a few of the subjects smoked cigarettes, and some were betel quid chewers (with tobacco), another major source of cadmium exposure. But the proportion of betel quid chewers was higher in the exposed group. In addition, the percentage of female subjects was higher in the exposed group (66.2%)than in the control group(30.8%).
Urinary cadmium is higher among women, as iron status and a number of pregnancies(during which body iron stores are often depleted)are important factors: low iron increases cadmium absorption(Akesson et al.,2002). Moreover, it has been reported that iron deficiency is a risk factor for increased blood and urine cadmium among never-smoking,pre-menopausal, non-pregnant women, independent of age, race, poverty, body mass index, and parity(Gallagher et al.,2011). Cadmium uses the same intestinal absorption transport system as zinc, calcium, and iron(Vesey,2010), three essential divalent cations. Iron (Fe)body stores were shown to especially influence the absorption rate of cadmium: the lower the Fe body stores, the more cadmium is absorbed from food in the intestinal tract (Ryu et al.,2004). Accordingly, the observed increase of urinary cadmium excretion in the exposed group compared to the control group in this study might be due to the above factors.
Regarding the source of cadmium exposure, it was reported that cadmium can enter the body primarily through food and smoking(Järup and Akesson,2009). The reason why this study population had increased urine cadmium levels is most probably due to food. According to a previous study by Kyi-Mar-Wai et al.(2017),chron-ic cadmium exposure was found in residents of Aye-yarwady Division in Myanmar. Therefore, we have done a pilot study on residents of Ta Zin Yae Kyae village of Nyaung Don Township in Ayeyarwady Division, Myanmar for exposure assessment and drinking water samples for cadmium source in this suspected area. We found that the cadmium level in the drinking water samples was below the detectable level. However, the determination of cadmium levels in several foods, including rice, or soils of the exposed area and the control area were not included in the present study. In Myanmar, rice is the staple food, and other rice-derived foods are also major components of daily meals. According to diet history, their daily consumed diet contained rice, rice-derived foods, potatoes, green leafy vegetables, and fish. Only a few of the subjects(12.3%) smoked cigarettes and 49.2% of the subjects in the exposed group were chew-ers of betel quid with tobacco, another major source of cadmium exposure. Furthermore, the study area(Ta Zin Yae Kyaw village), which is built on a freshwater lake, uses small boats for transportation and has no occupation-al history of cadmium contamination. Therefore, the dietary sources could be the potential source of cadmium contamination in that population.
Ayeyawady Division is a delta region of Myanmar, and Kyonpyaw Township plays a dominant role in the cultivation of rice, the products of which are distributed across the whole area of Ayeyawady Division. The residents in Nyaung Don Township in Ayeyawady Division also consumed rice produced in this area. Khin-Phyu-Phyu et al.(2017) studied the uptake and accumulation of As, Cd, Pb, Cr, Zn, Cu Ni Fe, and Mn heavy metals in rice grains, the soil, and tube well water in Kyonpyaw Township. They found that cadmium was detected in 6 out of 14 rice samples, but the levels were lower than the respective maxi-mum allowable concentration(MAC). In 14 soil samples,
the concentrations of cadmium were within MAC. Cadmium was detected in 14 out of 23 water samples, but 4 were above MAC(Cd=3 ppb, WHO,2006). Soil contamination with cadmium occurs mainly through pesticide, fertilizer, herbicide application, mining, or irrigation with contaminated groundwater (Egan et al.,2007).
In addition, fish is a major food in the diet in the study area. Nyaung Don Township is situated on the Ayeyawady riverside and the residents consume freshwater fish from the Ayeyawady River. Mar(2020) analyzed the uptake of cadmium in muscles of sampled fish with different feeding habits to compare levels of cadmium in fish from the Ayeyawady River, Myanmar with international standards. It was found that the fish samples were not fully safe for human consumption due to high levels of cadmium. Their study indicates that the high level of cadmium in muscle tissues of studied fish species may be due to anthropogenic activities such as municipal waste, and overuse of fertilizers, manures, and pesticides on farms along the Ayeyarwady River, as well as domestic wastes. Their findings highlight the presence of cadmium contamination in fish from the Ayeyawady River. Therefore, another route of exposure to cadmium in subjects in the present study might be through the consumption of fish contaminated with cadmium, accumulating in the human body.
In the present study, renal functions were assessed to study the effects of chronic cadmium exposure in apparently healthy Myanmar subjects because it has been reported that the kidney is the main target organ of cadmium in occupationally or environmentally exposed populations and in animals(Hong et al.,2004). Moreover, the evidence of a relationship between cadmium exposure and renal dysfunction is strongest(ATSDR,2012). Regarding renal function assessment, urinary β,-microglobulin (as a marker of tubular dysfunction), and serum creatinine and eGFR(as a marker of glomerular dysfunction) were determined in the present study.
It was found that urinary β,-microglobulin level was significantly higher in the exposed group compared to the control group (p =0.036). This finding was consistent with the findings of the study in China (Nordberg et al., 1997). They studied the biological monitoring of cadmium exposure and renal effects in a population group residing in a cadmium polluted area in China. They found that urinary β,-microglobulin level was 530ug/g creatinine (median) in the heavily exposed group(UCD, 10.7 ug/L)and 160 ug/g creatinine (median) in the medium exposed group (UCD,1.62 ug/L). They also reported a statistically significant dose-response relationship between urinary cadmium and β-microglobulin excretion in urine.
Similarly, the benchmark doses of cadmium exposure for cadmium-induced renal effects in a Thai population living in cadmium-polluted and non-polluted areas were examined, and it was found that the geometric means of urinary cadmium for all age groups in the polluted area (6.3 ug/g creatinine for men and 7ug/g creatinine for women) were significantly greater than those in the non-polluted area(0.5 ug/g creatinine for men and 1.1 μg/g creatinine for women). Urinaryβ,-microglobulin was also generally greater in the polluted areas(GM, 443 ug/g creatinine for men and 207.7 ug/g creatinine for women) than in the non-polluted areas(GM,249 ug/g creatinine for men and 187.2ug/g creatinine for women) for both men and women and all age groups(Nishijo et a., 2014). Likewise, subjects living in a cadmium-polluted area(UCD; median, 13.5ug/g creatinine)and a control area(UCD; median,3.1 ug/g creatinine)in China were investigated for the reference level of cadmium intake to induce renal dysfunction in a Chinese population. A significant difference was found in the level of urinary β-microglobulin between the polluted area and the control (300 ug/g creatinine vs 100 ug/g creatinine,p<0.01)(Chen et al, 2018).

In the present study, the median urinary β,-microglobulin excretion was significantly higher in the exposed group than that of the control group. In a clinical setting, urinary β,-microglobulin level above 1000 ug/g creatinine indicates damage to the proximal renal tubules (Aoshima, 1987; Nakagawa et al.,1993). When the results of the present study were evaluated in terms of this clinical cut-off level, no data was observed above this level in both groups.
Moreover, a significant positive correlation was found between urinary cadmium and urinary β,- microglobulin for all subjects(Spearman's rho=0.321,n=130. p<0.01)in the present study. When it was studied in the exposed group only, the correlation becomes stronger (Spearman's rho =0.347, n=65,p<0.01). It suggests that even in cases of chronic exposure to low-dose cadmium, urinary β,-microglobulin, a sensitive indicator of renal tubular dysfunction, was associated with the level of exposure to cadmium. This finding in the present study was in agreement with the previous finding (Hong et al..2004). They showed that there was a significant positive correlation between urinary cadmium and urinary β,-microglobulin(Spearman's rho=0.284,p <0.001)in a Chinese population. Similarly, urinary cadmium was significantly positively correlated with urinary β-microglobulin(Spearman's rho=0.189,p<0.01)in both men and women of the general Korean population (Eom et al.,2017).
Most likely, the subjects of the present study were from the general population with no occupational exposure to cadmium. Proximal tubular damage may be reversible and individuals can recover when cadmium exposure ceases in the general population. It is also a pre-clinical stage that does not indicate the presence of dis-ease. However, when renal tubular damage caused by cadmium is maintained continuously, it may progress to kidney dysfunction and decrease in the glomerular filtration rate (Jarup et al.,1998; Bernard,2008).
The present study also evaluated whether environmental cadmium exposure affects glomerular dysfunction in the study populations. The results showed that eGFR was significantly lower in the exposed group than in the control group(p =0.013). This was consistent with the finding of a study that was conducted on chronic occupational exposure to heavy metals(cadmium, lead, and chromium)and renal alterations in artisans and petrol hawkers in Nigeria. They found that eGFR was significantly lower in the exposed group (mean, 89.85 mL/min) than in the non-exposed group (mean, 99.31 mL/min)(p =0.000), the values of lower eGFR in the exposed group in their study being within the normal range(Bot et al.,2020).
In addition, there was a significant negative correlation between urinary cadmium and eGFR in all study groups in the present study(Spearman's rho =-0.257, p=0.003). A similar pattern but a stronger negative correlation was found in the exposed group only(Spearman's rho =-0.379,n=65,p<0.01). Likewise, a study of low-level cadmium exposure and kidney function in 167 living kid-ney donors in Sweden found that urinary cadmium (mean UCD,0.29 ug/g creatinine)was negatively correlated with eGFR(r=-0.33,p<0.005)(Wallinet al.,2014). Another study investigated the link between the toxicity of cadmium and clinical measure of kidney function, such as eGFR, in low and high cadmium-exposure areas in Thailand. They found that urinary cadmium (mean UCD,5.93 ug/g creatinine)showed a strong inverse association with eGFR (p<0.001)(Satarug et al.2018).
The findings in this study indicate that environmental cadmium exposure can induce renal dysfunctions; in both tubular and glomerular functions. It was reported that kid-ney tubular dysfunction, such as low molecular weight proteinuria, is an indicator of early adverse effects of cadmium exposure and progresses relatively slowly, and that kidney glomerular dysfunction appears at a later stage of chronic cadmium exposure(Jarup et al.,1998). Therefore, a systematic prospective cohort epidemiological study rather than a cross-sectional study would be necessary to evaluate the association between cadmium exposure and target organ diseases, such as kidney dysfunction in the general population.
In conclusion, the present study indicates that apparently healthy Myanmar people in the study area are exposed to low-level cadmium, which should be counted as a public health threat. We also found that cadmium exposure was associated with renal function changes in the study population. Further studies are necessary to evaluate cadmium exposure to the potential source of contamination in these areas of Myanmar and to determine cadmium-associated health effects in other organs.





