Part1: 3-Hydroxyphenylacetic Acid: A Blood Pressure-Reducing Flavonoid Metabolite
Mar 10, 2022
Contact: tina.xiang@wecistanche.com
Abstract: Regular intake of polyphenol-rich food has been associated with a wide variety of beneficial health effects, including the prevention of cardiovascular diseases. However, the parent flavonoids have mostly low bioavailability and, hence, their metabolites have been hypothesized to be bioactive. One of these metabolites, 3-hydroxyphenyl acetic acid (3-HPAA), formed by the gut microbiota, was previously reported to exert vasorelaxant effects ex vivo. The aim of this study was to shed more light on this effect in vivo and to elucidate the mechanism of action. 3-HPAA gave rise to a dose-dependent decrease in arterial blood pressure when administered i.v. both as a bolus and infusion to spontaneously hypertensive rats. In contrast, no significant changes in heart rate were observed. In ex vivo experiments, where porcine hearts from a slaughterhouse were used to decrease the need for laboratory animals, 3-HPAA relaxed precontracted porcine coronary artery segments via a mechanism partially dependent on endothelium integrity. This relaxation was significantly impaired after endothelial nitric oxide synthase inhibition. In contrast, the blockade of SKCa or IKCa channels, or muscarinic receptors, did not affect 3-HPAA relaxation. Similarly, no effects of 3-HPAA on cyclooxygenase nor L-type calcium channels were observed. Thus, 3-HPAA decreases blood pressure in vivo via vessel relaxation, and this mechanism might be based on the release of nitric oxide by the endothelial layer.
Keywords: flavonoids; gut microbiota;metabolite;3-hydroxyphenylacetic acid;blood pressure;vasorelaxation; coronary; artery; rat; pig

1. Introduction
Cardiovascular disease is the leading cause of death worldwide, with an estimated number of deaths approaching 18 million per year. Coronary artery disease and stroke contribute to approximately 85% of these fatal cardiovascular events [1]. Global mortality and morbidity have prompted the implementation of guidelines for the prevention of cardiovascular risks [2]. The detection of persistent high arterial blood pressure with subsequent treatment is among the main strategies[34]. Indeed, hypertension is classified as a major risk factor for cardiovascular diseases. It is mostly caused by increased systemic vascular resistance, and this is often related to various structural and functional changes in the vasculature, which disrupt vascular homeostasis. In particular, the tunica intima of blood vessels, formed by a single layer of endothelial cells, is dysfunctional. In addition, the vascular smooth muscle cells often appear more contracted and less responsive to endothelium-derived relaxing factors [5].
Several studies have provided evidence of the protective effects of a polyphenol-rich diet against cardiovascular diseases. Indeed, a diet rich in fruits, vegetables, nuts, chocolate, or tea, which are rich sources of flavonoids, has been associated with a reduction in the risk of cardiovascular diseases [6]. In addition to antioxidant, anti-inflammatory, antiplatelet, and antimicrobial properties, flavonoids also possess significant vasodilatory properties [7,8]. However, flavonoid intake worldwide is highly variable, and, once ingested, these compounds interact in a complex manner with the gastrointestinal tract. Briefly, flavonoids occur in plants mostly in the form of glycosides. After administration in the form of diet, they are hydrolyzed during digestion and this allows the release of the aglycone form in the small intestine. Aglycones, in turn, can undergo metabolism in the epithelium of the small intestine and later in the liver. This results in a very poor bioavailability of parent flavonoids, which was repeatedly confirmed [9,10]. However, the unabsorbed fraction passes from the small intestine into the distal gut, where it is cleaved by the colonic microbiota leading to the production of small phenolic compounds, including phenyl propionic, phenylacetic, benzoic acids, and hydroxy benzenes, which are subsequently absorbed [9]. It is noteworthy that over the last few decades, it has become clear that the protective effects of dietary flavonoids are attributed to their metabolites rather than their parent forms [10-12]. Notwithstanding, Booth and colleagues documented even in the early 1950s the presence of various flavonoid metabolites, namely 3,4-dihydroxyphenylacetic (DHPA), 3-hydroxyphenyl acetic (3-HPAA), and homovanillic acids in the urine of different animal species after oral ingestion of quercetin [13]; research on the biological effect of small phenolic metabolites of flavonoids is much more recent. Specifically, in recent years, research on the metabolic fate of flavonoids as well as studies reporting bioactivities of their microbe-derived metabolites has become a hot and intensively investigated topic in the field. Our research group has shown that several microbial metabolites, including DHPA,4-methyl catechol, and 3-(3-hydroxyphenyl) propionic acid, relax rat aorta is likely physiologically achievable concentrations [14,15]. To our best knowledge, 3-HPAA is one of the least explored metabolites. It was documented to be a metabolite of a number of phenolic compounds including different classes of flavonoids such as flavonols (quercetin with its glycoside rutin, kaempferol), isoflavones, and flavanols (both oligomeric procyanidins and their monomeric units, catechin and epicatechin) (Figure 1) [16-20].

As 3-HPAA relaxes smooth muscle cells ex vivo [14], this study aimed to test if this metabolite is able to cause a decrease in arterial blood pressure in vivo and to detect its mechanism of action in a series of mechanistic experiments.

2. Materials and Methods
2.1. Animals
The in vivo experiments were carried out on spontaneously hypertensive rats(SHR)obtained from the Czech Academy of Sciences, Prague, Czech Republic. The animals were bred in the animal facility of the Faculty of Pharmacy and maintained at a constant temperature of 23-25°C with a 12 h dark/light cycle. Rats were provided a standard diet and tap water ad libitum. The study (reg. No.4937 2019-9) was approved by the Ministry of Education, Youth and Sports, conforming to The Guide for the Care and Use of Laboratory Animals published by the US National Institutes of Health (8th edition, revised 2011, ISBN-13:978-0-309-15400-0).
2.2.Chemicals
Pentobarbital, sodium nitroprusside, dimethyl sulfoxide (DMSO), L-Nw-nitro arginine methyl ester(L-NAME), atropine, TRAM-34/1-[(2-chlorophenyl)diphenylmethyl]-1H-pyrazole, indomethacin, nifedipine, bradykinin, KCl, CaCl, and UCL-1684/6,12,19, 20,25,26-hexahydro-5,27:13,18:21,24-trietheno-11,7-metheno-7H-dibenzo[b,m][1,5,12,16]tetraazacyclotricosine-5,13-dium trifluoroacetate hydrate were purchased from Sigma-Aldrich(Steinheim, Germany). Bay K8644 was obtained from Axon Medchem BV(Groningen, The Netherlands). The tested metabolite 3-HPAA was purchased from Toronto Research Chemicals(Toronto, ON, Canada). NaCl, NaHCO3, and D-glucose were pro-vided by PENTA s.r.o (Prague, Czech Republic).MgSO4.7H2Owas purchased from Erba Lachema s.r.o.(Brno, Czech Republic),and KH2PO4 from Dr. Kulich Pharma s.r.o. (Hradec Kralové, Czech Republic). Saline was purchased from Baxter Czech spol. s.r.o.(Prague, Czech Republic) and heparin from Zentiva (Prague, Czech Republic).
Sodium nitroprusside, L-NAME, and atropine were dissolved in distilled water. Stock solutions of TRAM-34(1 mM) and UCL-1684(100 μM) were prepared as water solutions supplemented with 20% and 10% DMSO, respectively. A stock solution of indomethacin (1 mM)was also prepared in 10%DMSO/water, and Bay K8644(10 mM) and nifedipine (10 mM) were dissolved in pure DMSO. The final concentration of DMSO in the tissue chamber was always<0.2%.The Krebs solution contains the following (mM): NaCl119, KCl4.7, CaCl2 1.25,KH2PO41.18, MgSO4.7H2O1.17, NaHCO325, and D-glucose 11.
2.3.In Vivo Experiments
Twelve SHR rats (average weight 356 ± 21 g, blood pressure under anesthesia 211±64/152±45 mmHg, heart rate 381 ± 37 bpm) were anesthetized i.p. by pentobarbital (50 mg. kg-). The pressure transducer MLTO380/D was linked to the left common carotid artery, and arterial blood pressure with heart rate was recorded using a Power Lab device connected to the LabChart 7 software(ADInstruments, Sydney, Australia). The left saphenous vein was cannulated for i.v.administration of a bolus or an infusion After surgery, each rat was allowed to stabilize for 15 min before the experiment. 3-HPAA was dissolved in saline and administered under two protocols:(1) as a single bolus dose ranging from 0.001 to 10 mg kg-1(the volume applied was always 0.1 mL, n=8); or (2) as four subsequent 5 min-lasting infusions at doses 0.05, 0.25,1 and 5 mg.kg-1.min-1 (n=4) in the infusion rate of 50μL per minute using the"Genie" Kent syringe pump (Kent Scientific Corporation, Torrington, CT, USA)(Figure 2a). In both protocols, the next dose was always given after blood pressure was stable for at least 5 min. As a control, each animal was treated with saline under the same conditions before the first administration of 3-HPAA was carried out. After the measurement, each rat was sacrificed by i.v. KCl(1 mL, 1 mol·L-). The body temperature during the experiment was maintained at 36.5± 0.5°C using a heating plate.


2.4.Ex Vivo Experiments
2.4.1.Tissue Preparation
The ex vivo experiments were performed on porcine coronary arterial ring segments (Figure 2b). Porcine hearts (n= 11)were obtained from a local slaughterhouse. Pigs were healthy animals of both sexes, from standard breeding and under veterinary control, intended for consumption. The hearts were processed for the experiment approximately 4 h after the slaughter of the animal. The hearts were immersed in the Krebs solution, and the left circumflex coronary artery was immediately excised, again immersed in the Krebs solution and cleaned of adherent fat, connective tissue, and blood. Afterward, the purified coronary artery was cut into cylindrical rings of approximately 3 mm in length. For certain mechanistic experiments, the endothelial layer was mechanically disrupted by gently rubbing the luminal surface with forceps. The rings were maintained in tissue baths filled with the Krebs solution under oxygenated conditions (95% O, and 5% CO2)at 37 °C. Each artery ring was hung between two stainless-steel wire hooks, one of them fixed to a holder and the second connected to a transducer and computer equipped with S.P.E.L. Advanced Kymograph Software, v3.2(Experimetria Ltd., Budapest, Hungary). This arrangement enables the measurement of isometric tension. The preparations were equilibrated at a tension of 2 g for 40 min, during which the Krebs solution was replaced every 10 min After that, the tension was set at 1g (baseline), each tissue bath was filled with 5mL of the Krebs solution, and the following viability test was performed: the coronary rings were contracted with KCl(final concentration inside the bath was 40 mM), and when the plateau was attained, bradykinin (300 nM) was added to confirm intact endothelium or denuded rings. Then, the coronary rings were washed several times with the Krebs solution.
2.4.2. Confirmation of the Vasodilatory Activity of 3-HPAA on the Porcine Coronary Artery
The vasorelaxant activity was measured on KCl-precontracted (40 mM) arterial rings (Figure2b). Once the plateau had been reached,3-HPAA was cumulatively added to the bath in concentrations ranging from 100 μM to 1 mM.3-HPAA was prepared in the Krebs solution. The Krebs solution without the tested compound was added to some coronary rings as the control using the same procedure. Each dose was applied after stabilization of the relaxant response caused by the previous dose, and sodium nitroprusside (100 μM)was used to induce maximal relaxation in all experiments at the end of the procedure.
2.4.3. Mechanistic Experiments
In the following experiments, the mechanism of vasodilatory action of 3-HPAA was studied on intact endothelium coronary rings using nitric oxide (NO) synthase inhibitor, L-NAME(100 μM); a muscarinic receptor antagonist, atropine (50 μM); a cyclooxygenase (COX) inhibitor, indomethacin (10 μM); or the intermediate and small conductance Ca2+-activated Kt channels inhibitors, TRAM-34(10 μM) and UCL-1684 (1 μM), respectively (Figure 2b). Atropine or inhibitors were always added 30 min before the addition of KCl (40 mM). Afterward, in a separate experiment, the involvement of vascular Cay1.2 Ca2+channels (L-type) on 3-HPAA-induced vasorelaxation was investigated by pre-treating endothelium-denuded coronary rings with 15 mM KCl followed by incubation with the 3-HPAA at a concentration of 1 mM for 30 min. Then, an L-type calcium channel activator, Bay K8644, was applied cumulatively (100 pM-10μM)in the dark, to induce a contractile response. KCl(80 mM) was used to induce maximal contraction. Rings incubated with the corresponding volume of the vehicle (the Krebs solution) were used as negative controls. In addition, rings incubated with the known L-type calcium channel inhibitor nifedipine (150 nM) were used as positive controls. The investigated target proteins and the ligands used in the mechanistic experiments are summarized in Table 1.
 mechanistic studies and the ligands used in the ex vivo experiments on the porcine coronary artery")
2.5. Data Analysis
GraphPad Prism 7.03 (GraphPad Software, San Diego, CA, USA) was used for data analysis. For in vivo experiments, differences between individual bolus doses of 3-HPAA and control (saline) were compared using a one-way ANOVA, followed by the Dunnett post hoc test. For infusions, a two-way ANOVA followed by the Dunnett post hoc test was employed. For the mechanistic ex vivo experiments, the results were compared by using an unpaired t-test. For experiments with Bay K8644, two-way ANOVA was used followed by a Dunnett test for multiple comparisons. Data are shown as mean ± SEM.

3. Results
3.1.Effect of 3-HPAA on the Blood Pressure and Heart Rate In Vivo in SHR
3.1.1. Single Bolus Administration
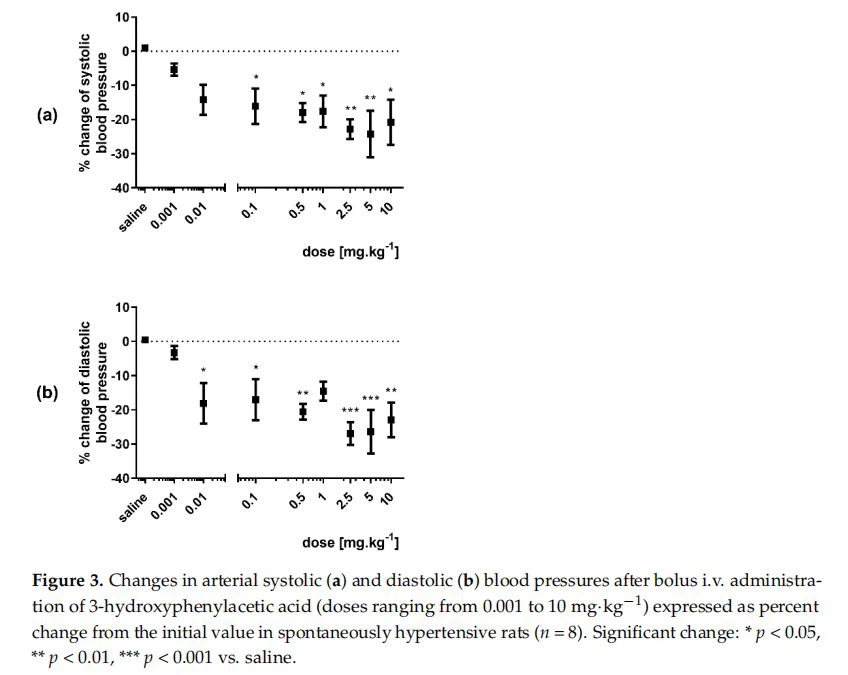
A significant decrease in mean, systolic, and diastolic blood pressures was observed after bolus administration of 3-HPAA in doses ranging from 0.01 to 10mg.kg-'(Figures 3 and S1). The decrease in systolic blood pressure was apparent from a dose of 0.1 mg. kg-I(Figure 3a), whereas diastolic blood pressure dropped significantly even from a 10 times lower dose (0.01 mg. kg-')(Figure 3b).In the same experiment, no effect on heart rate was found at any of the 3-HPAA doses (Figure S2).
3.1.2. Infusion Administration
The 5 min-lasting infusions of 3-HPAA resulted in a decrease in mean, systolic, and diastolic blood pressures(complete results in Figure S3). The effect was dose-dependent, reaching maximally approx. 50%. Significant changes were produced by the two highest doses, 1 and 5 mg·kg-1.min-I(Figure 4). Additionally, in this case, no significant changes in heart rate were found (Figure S4).
3.2. Confirmation of the Vasodilatory Properties of 3-HPAA on Porcine Coronary Artery
In ex vivo experiments, 3-HPAA induced vasodilation of pig coronary artery in a dose-dependent manner(Figure 5). Except for the first dose, vasodilation was observed. The results were, however, significant only for the highest concentration(1 mM). The same concentration was used for further mechanistic testing ex vivo.
infusions on systolic blood pressure(a) and diastolic blood pressure(b)in spontaneously hvpertensive rats (n =4). Significant change: p<0.05.")
in porcine coronary arterial rings (n =6).Data are expressed as % from the maximal relaxation induced by sodium nitroprusside(100 uM).Significant change:***p<0.001 vs.control, ns—not significant.")
3.3. Mechanism of the Vascular Effects of 3-HPAA Studied Ex Vivo on Porcine Coronary Artery
To investigate the mechanisms underlying the 3-HPAA-induced vasodilation, we compared its effects on endothelium-intact and endothelium-denuded porcine coronary arterial rings precontracted with KCl. The endothelium removal decreased the vasodilatory effect (Figure 6b). Following on from this finding, the involvement of endothelial NO was tested. Pre-treatment with an inhibitor of eNOS, L-NAME (100 uM), also resulted in a significant decrease in 3-HPAA-induced vasodilation (Figure 6c). In contrast, analogous pre-treatment of coronary rings with muscarinic receptor antagonist atropine (50 uM), or with IKCa or SKCa channel blockers, TRAM-34(10 μM) and UCL-1684(1 μM), respectively, or with the COX inhibitor, indomethacin (10 μM) did not cause any changes in vasodilation produced by 3-HPAA(Figure 6d-g). Finally, we decided to investigate whether 3-HPAA may act through inhibition of Cay1.2 calcium channels(L-type)on vascular smooth muscle cells. Pre-treatment of the rings with 3-HIPAA(1 mM) had no significant effect on contraction induced by cumulative doses of Bay K8644(100 pM-10 μM)(Figure 7), while incubation with the known Cav1.2 calcium channel (L-type) inhibitor nifedipine(150 nM) significantly reduced the contractions (positive control).
. Scheme of the representative isometric tension traces of the porcine coronary arterial rings (a). Ex vivo vasodilatory effects of 3-HPAA (1 mM) were evaluated on endothelium-intact E(+) and endothelium-denuded E(−) porcine coronary arterial rings precontracted with KCl (40 mM) (b). In another experiment set, intact coronary rings were used and the percentage of relaxation was evaluated in the presence of: NO-synthase inhibitor L-NAME (100 µM) (c), or the M-receptor antagonist atropine (50 µM) (d), or Ca2+-activated K+ channel inhibitors, TRAM-34 (10 µM) (e), or UCL-1684 (1 µM) (f), or the cyclooxygenase inhibitor indomethacin (10 µM) (g). Data were calculated from the maximal relaxation induced by sodium nitroprusside (100 µM). Significant change: * p < 0.05, ** p < 0.01, *** p < 0.001 (n = 6, for control n = 4), ns—not significant.")
. Effect of pre-treatment of coronary rings with 3-hydroxyphenylacetic acid (3-HPAA, 1 mM)on contraction induced by cumulative doses of the L-type calcium channel activator, Bay K8644 (100 pM-10μM). Nifedipine(150 nM) and vehicle(the Krebs solution) were used as positive and negative controls, respectively (b). Data were calculated from the maximal contraction induced by KCl(80 mM).Significant change:*p<0.05,**p<0.01 vs.the control (n=7 for 3-HPAA, for both controls n=4).")
Click the link for part2 further information
https://www.xjcistanche.com/news/part2-3-hydroxyphenylacetic-acid-a-blood-pre-54725696.html





